Articles for Physicians - Articles by Doctors › Case Reports › Portal Venous System Thrombosis Following Splenectomy
INTRODUCTION:
Portal venous system thrombosis (PVST) following splenectomy due to trauma is rare. Due to the infrequent nature of this event, few studies have been completed to create standards of care for these patients. When to screen for, and how to manage this condition remains understudied. Indeed portal venous thrombosis is a life threatening emergency, and a review of the risk factors, and frequency of this event is important. This paper describes an interesting case of splenectomy following trauma, its rare complication of PVST, and finally discusses the data available regarding screening and treatment.
CASE REPORT:
A.M. is a 34 year old Caucasian female who was admitted to the emergency department following a high speed head on motor vehicle collision so severe that the vehicles steering wheel was found in the road. The patient admitted to have fallen asleep while driving to pick up her boyfriend. The patient arrived via ambulance reporting severe left upper quadrant pain, 10/10 in intensity. Vital signs on arrival were as follows: Blood Pressure: 120/49, Pulse: 110, Respirations: 32, Oxygen saturation: 97% on room air. On physical exam the patient was alert awake and oriented times 3, and in moderate distress due to pain. The patient’s skin was pale, and there were multiple areas of abrasion on her face, forehead, elbows and legs. The patient’s anterior chest was reproducibly tender to palpation bilaterally, and on the left lateral side. No abrasions were found on the neck, and no focal motor or sensory deficits were noted. Hemoglobin and hematocrit in the ED were 10.4 and 36 respectively. Platelet count on admission was 258,000/mm3.
The patients’ medical history includes attention deficit disorder, anxiety, bipolar disorder, post traumatic stress disorder, obsessive/compulsive disorder, asthma, migraines, hepatitis C, and polysubstance abuse. Past surgical history is positive for a tubal ligation. Family history is noncontributory. Social history reveals tobacco usage of 1.5 packs per week and denial of alcohol or illicit drug use.
The patient underwent routine trauma evaluation, including CT scans of head, c-spine, chest and abdomen/pelvis. The head and c-spine evaluations were negative, while the chest and abdomen imaging revealed a high grade (IV-V) splenic laceration with active extravasation and associated hemoperitoneum, mid-right hepatic lobe laceration, and multiple small bowel contusions without visible free air appreciated in the peritoneal cavity.
Shortly after returning to the emergency department, the patient began to show signs of hemodynamic instability, with her lowest blood pressure documented as 62/48, but was responding to infusion of crystalloid and one unit of packed red blood cells. She was transported to the operating room for emergent exploratory laparotomy. Confirmation of splenic laceration was made, and total splenectomy was performed. The spleen was completely subdivided. Diligent examination of the liver and small bowel failed to reveal any further noteworthy complications. An estimated 1.5 liters of blood was found in the abdominal cavity. The patient tolerated the procedure well, without episodes of hypotension or hypoxia, and had an uncomplicated hospital stay of 7 days.
Two days following discharge (postoperative day 9) the patient presented to the emergency department complaining of increased abdominal pain and distension. The pain was described as 10/10 in severity, constant, sharp, and located primarily in her lower abdomen. The pain had reportedly begun one day prior. The patient stated that she had a fever of 101.5 degrees Fahrenheit. Furthermore, she reported nausea without vomiting, and denied shortness of breath, chest pain, dysuria, or hematuria. Her last bowel movement and flatus was two days prior to this admission. On physical examination, the patient was alert and oriented x 3, slightly tearful and appeared uncomfortable. Abrasions from here previous car accident were still visible on her forehead. The abdominal exam revealed a moderately distended diffusely tender to palpation abdomen that was tympanitic to percussion. There was no rebound tenderness or guarding. Bowel sounds were hypoactive. Her incision was clean, dry, and intact, without erythema, edema, or induration. Extremities were warm and well perfused. No focal neurological deficits were appreciated. Laboratory workup included: Hematocrit 32, WBC 12.9, Platelets 735, liver function tests within normal limits. CT scan of abdomen and pelvis revealed extensive thrombus of the residual splenic vein extending to involve the entire portal vein and the proximal superior mesenteric vein. Scant free fluid was also seen in the abdomen. The patient was admitted under surgical service and begun on Heparin drip, followed by transition to oral Coumadin anticoagulation therapy. She was discharged four days later when a therapeutic INR was maintained, and abdominal discomfort was minimized. The patient continues to have weekly blood workups, to ensure appropriate anticoagulation. The patient had a followup CT scan of the abdomen on POD 33 which showed marked improvement of the portal venous system thrombosis.
DISCUSSION:
The reported incidence of portal venous system thrombosis following splenectomy varies from 7-55% depending on the methods of removal and comorbid disease. For example, Ikeda et al. reported a 55% incidence of PVST following laparoscopic splenectomy, versus 19% in open splenectomy. Petit et al. reported a 7% incidence of splenic vein thrombosis in a retrospective study involving 183 patients who received routine imaging to screen for thrombosis post splenectomy. Yet, this study included patients who underwent splenectomy for various issues, not only trauma. Indeed only 34 of 183 splenectomies were for trauma, the majority of the rest being for various hematological disorders. In this study 12 of the 13 patients who were found to have splenic vein thrombosis also had an associated hematologic disorder. Thus, the true incidence of PVST following splenectomy due to trauma proves to be elusive. When excluding for oncologic neoplasm and laparoscopic splenectomy the true incidence is likely closer to 5-15%. Due to the potential lethality of portal venous system thrombosis, it would be ideal to have guidelines regarding screening. Some clinicians have suggested regular screenings for PVST following splenectomy, for example one week post-op (Tran et al.). van’t Reit et al. and Stella et al. accurately observe that physicians must have a high level of suspicion and that any post splenectomy patient with abdominal pain and fever should undergo at least color Doppler ultrasonography of the portal venous system.
DIAGNOSIS:
The diagnosis of this complication can be made by CT with IV contrast, CT angiography, Doppler ultrasonography, magnetic resonance angiography, and arterial portography or splenoportography. (6) The method used depends on accessibility and stability of the patient. The use of contrast material is contraindicated in renal insufficiency, and those with allergies to certain seafood. The most commonly used modes are CT with contrast and Doppler ultrasound. Sensitivity of Doppler ultrasonography for this condition is reported as around 80%, whereas CT sensitivity is over 90%. (10)
ETIOLOGY:
There are many factors affecting the pathophysiology of portal venous system thrombosis following trauma. The trauma victim suffers from insults and aggravating factors which encourage a hypercoagulable state. Vessel wall injury, hypoxemia, venous stasis, immobility, and clotting mechanism abnormalities are all factors documented to play a role in hypercoagulability following trauma. (4) Regarding a specific cause of portal venous system thrombosis following splenectomy for trauma, one major factor may be the splenic vein stump. Certainly, one can presume, that due to the lack of flow in the stump following splenectomy a thrombus will form. This thrombus may then propagate further into the portal venous system, leading to significant complications. Yet, why some persons develop further thrombus propagating from this origin and others do not remains a mystery. Examination for abnormalities in the clotting mechanism should certainly be performed in any person with this condition. Another preventive measure, albeit theoretical, would be to dissect the splenic vein proximally during the surgery to the first perforating pancreatic branch, and ligate the vessel at the point immediately distal to the perforating branch. This would create less of nidus for thrombus formation. An additional concern that has been voiced in the past is that the frequent thrombocytosis seen following splenectomy may have a causal relationship with portal venous system thrombosis. The studies are conflicting. Stamou et al. did find a correlation between a platelet count and risk of thrombosis, namely that a platelet count over 650,000/mm3 was indeed a risk factor for thrombosis. Whereas Slater and Sherlock, whom evaluated 318 patients who underwent splenectomy (75% of which developed thrombocytosis) were unable to find correlation between the two.
TREATMENT:
The treatment of PVST presents a challenge in that some form of anticoagulation will need to be administered to an individual who has recently had a major surgery. As stated above, if PVST occurs it will likely manifest at around one week post-op. (Tran et al) Therefore, the risks of anticoagulation should be minimal. Indeed, current recommendations for heparin or low molecular weight heparin state that heparin resumption should be at least twelve hours after a major surgery, and should be delayed longer if there is any evidence of bleeding. (1) The importance of treating a patient with mesenteric venous thrombosis was documented by Naitive and Weissman, who reported zero deaths in those patients who received systemic anticoagulation, while they reported a morality rate of 50% in uncoagulated patients.
Parker et al. describe using thrombolytic therapy through an indwelling SMA catheter, followed by systemic chemical anticoagulation, with good affect. The patient described in the vignette above was begun on a heparin drip, and transitioned to oral anticoagulation, without further complication to date. The decision regarding how long anticoagulation should be continued, and when/if followup imaging is appropriate is unknown. A review article on the treatment of portal vein thrombosis suggests using the management regime for DVT in the lower extremities, i.e. 3-6 months. (3,14) Continued long term therapy is justified in patients with prothrombotic tendencies, or extensive thrombosis of the portal venous system.(14) The final decision of length of treatment may rely on follow-up imaging studies.
CONCLUSION:
The possibility of portal venous system thrombosis following splenectomy mustn’t be overlooked, as the consequences can be dire. Unfortunately, there are no current guidelines in place regarding screening and treatment for this condition. Physicians must diligently evaluate a patient’s history and carry a high level of suspicion when treating patients with abdominal pain and fever, who have recently had a splenectomy. Doppler ultrasonography and CT scan with IV contrast are both effective and rapid modes of diagnosis. Patients who are diagnosed with this condition must begin either thrombolytic or anticoagulation therapy as soon as possible, in order to avoid life threatening ischemic bowel. The duration of anticoagulation treatment should be at least three months, and lifelong treatment is recommended for those who have associated hypercoagulable conditions.
*Note: The author will gladly email CT images relating to this case to further the educational capacity of this article.
References
1. Gregory, YH Lip. Management of Anticoagulation before and after elective surgery. Uptodateonline.
2. Moore, Ernest, David Feliciano, and Kenneth Mattox. Trauma. 5th. New York: McGraw-Hill, 2004. 663-683. Print.
3. Hirsh J and Lee AY. How we diagnose and treat deep vein thrombosis. Blood. 2002 May 1;99(9):3102-10.
4. Ikeda M, Sekimoto M, Takiguchi S, et al. Total splenic vein thrombosis after laparoscopic splenectomy: a possible candidate for treatment. American Journal of Surgery. 2007 Jan;193(1):21-5.
5. Naitove A, Weissman R. Primary mesentaric venous thrombosis. Annals of Surgery. 1965; 161:516-523.
6. Nawaz, Ali. Portal Vein Thrombosis. Online: http://emedicine.medscape.com/article/373009-overview
7. Parker H, Bynoe R, and Nottingham J. Thrombosis of the Portal Venous System after Splenectomy for Trauma. Journal of Trauma. 2003; 54:193-196.
8. Petit P, Bret PM, Atri M, et al. Splenic vein thrombosis after splenectomy: frequency and role of imaging. Radiology. 1994 Jan; 190(1):65-8.
9. Romano F, Caprotti R, Conti M, et al. Thrombosis of the splenoportal axis after splenectomy. Langernbecks Archives of Surgery. 2006 Sep; 391(5):483-8.
10. Slater PP, Sherlock EC. Splenectomy, thrombocytosis, and venous thrombosis.
American Surgery. 1957; 23:549-554.
10. Sogaard K, Astrup L, Vistrup H, and Gronbaek H. Portal vein thrombosis; risk factors, clinical presentation and treatment. BMC Gastroenteroogy. 2007
7:34.
11. Stamou KM, Toutouzas KG, Kekis PB, et al. Prospective study of the incidence and risk factors of postsplenectomy thrombosis of the portal, mesenteric, and splenic veins. Archives of Surgery. 2006 Jul;141(7):663-9.
12. Stella M, Serventi A, and Friedman D. Right portal vein thrombosis after splenectomy for trauma. Journal of gastrointestinal Surgery. 2005 May- Jun;9(5):646-7.
13. Tran T, Demyttenaere SV, Polyhronopoulos G, et al. Recommended timing for surveillance ultrasonography to diagnose portal splenic vein thrombosis after laparoscopic splenectomy. Surgical Endoscopy. 2009 Dec 29. [Epub]
14. Webster G, Burroughs A, and Riordan S. Review article: portal vein thrombosis- new insights into aetiology and management. Alimentary Pharmacological Therapy. 2005; 21:1-9.
Article By: John Richey
Causes and Treatment of Stress
Haiti - Medical Cataclysm
Miller Fisher Syndrome: A Case Report
A Case of Abruptio Placentae with a History of H1N1 Influenza Infection
An interesting case of Hypokalemic periodic paralysis
Fracture of malleus and dislocation of multiple ossicular joints after welding flame burn
Erythema induratum: a case of mistaken identity
Fracture of malleus and dislocation of multiple ossicular joints after welding flame burn
A liver fibrosis cocktail? Psoriasis, methotrexate and genetic hemochromatosis
Acute unilateral hearing loss as an unusual presentation of cholesteatoma
An interesting case of Hypokalemic periodic paralysis
A Case of Abruptio Placentae with a History of H1N1 Influenza Infection
Bilateral neuro-retinitis following chick embryo cell anti-rabies vaccination – a case report
Erythema induratum: a case of mistaken identity
splenectomy and hypercoagulable state trauma
,post splenectomy portal vein thrombosis
, portal vein thrombosis after splenectomy, post splenectomy thrombosis, portal vein thrombosis post splenectomy, portal vein thrombosis due to splenectomy,splenectomy portal vein thrombosis
,portal vein thrombosis heparin gtt
, ,splenectomy splenic vein thrombosis
,splenectomy in portal vein thrombosis
,splenic vein thrombosis post splenectomy
,recurring venous thrombosis following laprascopic splenectomy
, , ,splenectomy causing hypercoagulation
,portal thrombosis after splenectomy
, , ,duration of anticoagulation for splenic vien thrombosis post splenectomy
,portal venous system thromboses
,post spleeectomy portal vein thrombosis
,erythema following the venous system
,portal vein thrombosis following splenectomy
,splenectomy and develop portal vein thromboais
,medscape splenectomy thrombolytic therapy
,potal vein throbosis after splenectomy
,portal vein thrombosis treatment kids
,hepatic venous thrombosis post splenectomy
,splenic veinthrombus s p splenectomy
,splenic vein post splenectomy on ultrasound
,post splenectomy complication thrombosis
, , , ,splenectomy followed by portal vein thrombosis with severe thrombocytosis
,portal vein thrombosis with spleenremoval
,spleniv vein thrombosis following splenectomy
,complications of splenic portal vein thrombosis
, ,venous thrombosis and splenectomy
,splenectomy causing portal vein thrombosis
,cause of portal vein thrmobosis post splenectomy
,portal vein thrombosis after splenctomy
,continued portal vein is sues after splenectomy
,sesitivity of multi detector ct in portal vein thrombosis
,propagating splenic thrombosis
, , , ,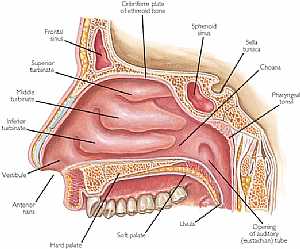 Nose anatomy
Nose anatomy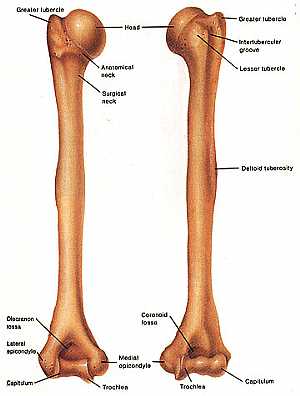 Humerus bone
Humerus bone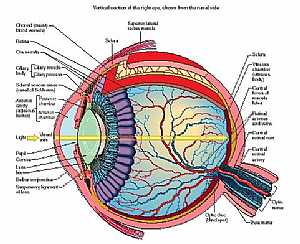 Eye anatomy
Eye anatomy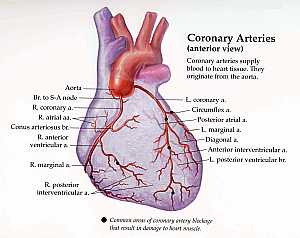 Coronary arteries anatomy
Coronary arteries anatomy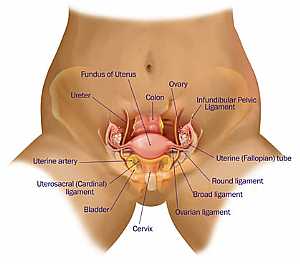 Female pelvic anatomy
Female pelvic anatomy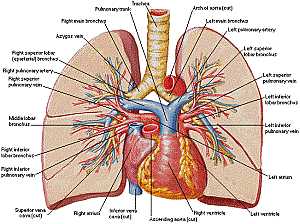 Heart and lung anatomy
Heart and lung anatomy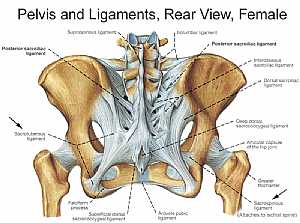 Bones and ligaments of the FEMALE Pelvis
Bones and ligaments of the FEMALE Pelvis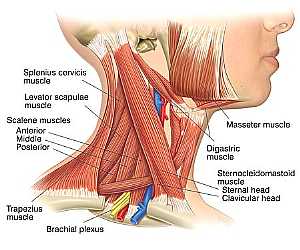 Neck Anatomy
Neck Anatomy MidBrain anatomy
MidBrain anatomy Oral Cavity
Oral Cavity Stomach anatomy
Stomach anatomy Lung anatomy
Lung anatomy Basal Cell Carcinoma ("Rodent Ulcer" Type)
Basal Cell Carcinoma ("Rodent Ulcer" Type)
 Basal Cell Carcinoma ("Rodent Ulcer" Type)
Basal Cell Carcinoma ("Rodent Ulcer" Type) Basal Cell Carcinoma (Histology-Morpheaform Type)
Basal Cell Carcinoma (Histology-Morpheaform Type)
 Basal Cell Carcinoma (Histology-Morpheaform Type)
Basal Cell Carcinoma (Histology-Morpheaform Type) Basal Cell Carcinoma (Histology-Nodular Type - High power)
Basal Cell Carcinoma (Histology-Nodular Type - High power)
 Basal Cell Carcinoma (Histology-Nodular Type - High power)
Basal Cell Carcinoma (Histology-Nodular Type - High power) Basal Cell Carcinoma (Histology-Nodular Type- High power)
Basal Cell Carcinoma (Histology-Nodular Type- High power)
 Basal Cell Carcinoma (Histology-Nodular Type- High power)
Basal Cell Carcinoma (Histology-Nodular Type- High power) Skin
Skin
 Skin
Skin Nervous System -- Basic
Nervous System -- Basic
 Nervous System -- Basic
Nervous System -- Basic Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy Head anatomy
Head anatomy
 Head anatomy
Head anatomy Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy© Copyright 2001-2022 eDoctorOnline.com
Be the first one to comment on this article!