Articles for Physicians - Articles by Doctors › Medical Articles › Hypoxia: Deadly killer in Anesthesia
History of oxygen:
Colorless, odorless diatomic gas discovered by Priestley in 1771 which is manufactured by fractional distillation of air. 21% volume of Atmospheric air is occupied by oxygen. Other gases are:
Atmospheric Air
¨ Nitrogen 78.00%
¨ Oxygen 21.00%
¨ Co2 0.03%
¨ Others 0.97%
Despite of some dark sites oxygen is essential for cellular respiration. This oxygen is transported from air to mitochondria of a cell via series of steps by changing its partial pressure. This gradual change of partial pressure of oxygen up to mitochondria has been termed as oxygen cascade.
Oxygen Cascade.
Partial pressure at different levels mm of Hg
Dry atmospheric gas ( PiO2) 160
Humidified alveolar gas (PAO2) 106
Po2 in Venous end of Pul. Capillary 100
Systemic Artery (PaO2) 95
Po2 in ISS 40
Po2 within the cell 23
Reduction in the partial pressure of oxygen in the cascade may lead to marked reduction of partial pressure in mitochondria and if pressure falls below a critical level Anaerobic metabolism occurs in the body. This critical point of mitochondrial PO2 has been termed as Pasteur Point. It is about 0.15-0.3 kPa
Oxygen Transport
Oxygen is transported in the blood by two ways:
- In dissolved form which constitutes 3% of total oxygen volume and
- In combination with Hb which constitutes about 97% of total volume of oxygen
Dissolved in plasma (3%)
0.003 ml/mm of Hg/dl of blood
Dissolved state of oxygen in the blood is determined by Henry’s law. About 0.3 ml of oxygen is dissolved in100 ml of blood at 95 mm of Hg.
It is responsible for Po2 in the blood.
In combination with Hb (97%)
- About 1.34 ml of O2 can combine with 1 gm of Hb at 100 mm of Hg at 37°c
- arterial blood contains about 19.8 ml O2/dl of blood
- venous blood contains about 15.2 ml O2/dl of blood
So under normal condition tissue removes average 5 ml O2 per dl of blood. Therefore body consumes average 250 ml O2 per min.
Our body operates in a very low oxygen environment and it will take about 3-4 minutes to burn total O2 volume of blood for Aerobic metabolism. So optimum functioning of oxygen cascade is essential for optimum tissue oxygenation. Otherwise body will experience reduced oxygenation at tissue level. This has been termed as hypoxia.
Hypoxia
Oxygen deficiency at tissue level
Or
Reduced oxygen for tissue respiration
Hypoxia has been classified in many ways. But there are basic four types of hypoxia.
Types:
- Hypoxic
- Anaemic
- Histotoxic
- Stagnant
Hypoxic Hypoxia
Reduced oxygen tension in the blood.
Hypoxic hypoxia is also called hypoxaemia when Po2 <80 mm of Hg.
Causes:
Alveolar hypoventilation
-drug overdose
-COPD exacerbation
pulmonary diffusion defect
-pulmonary fibrosis
-Emphysema
-pulmonary oedema
Pulmonary V/Q mismatch
-Asthma
-pulmonary embolism
R-L shunt
- Atelectasis
- Cyanotic congenital heart disease
? FiO2 or PBaro
Anaemic
In anaemic hypoxia PaO2 is normal but there is insufficient amount of functional hemoglobin to carry O2
Occurs in Anaemia and CO poisoning
In anemic hypoxia we should correct anaemia first before going oxygen therapy because-
- 50% reduction of Hb causes 50% reduction in CaO2 but
- 50% reduction of PaO2 causes 18% reduction in CaO2
Stagnant
Also called Ischaemic hypoxia
Here Hb conc. and Po2 are normal but there is slower blood flow to the tissue
Occurs in –CCF
-Atherosclerosis
Histotoxic
In Histotoxic hypoxia
-PaO2 is normal
-Hb conc. is normal
-supply of O2 to the tissue is normal
-But tissue can’t utilize supplied O2
Occurs in –
Cyanide poisoning
Chronic CO poisoning
Sign and Symptoms
Successful treatment of tissue hypoxia requires early recognition. This can be difficult because the clinical features are often non-specific and include-
CNS
Nausea
Headache
Drowsiness
Confusion
Convulsion
Unconsciousness
Hb Saturation
85%------- Mental impairment
75%-------- Severe Mental impairment
65%-------- Unconsciousness
Respiratory
Hyperventilation
Pulmonary HTN
Kidney
Function impaired
CVS
Tachycardia
Bradycardia
Arrythmia
Asystole
We should be aware of cyanosis. Cyanosis is something when it is present but if it is absent it doesn’t mean anything about oxygenation status. It may be absent in-
¨ Anaemic hypoxia(5gm% deoxygenated blood required)
¨ CO poisoning
¨ Histotoxic hypoxia
Cell injury and Hypoxia
¨ The first point of attack of hypoxia is the cell’s aerobic respiration
¨ If Partial pressure of oxygen in the tissue reaches to a level below Pasteur Point it starts Anaerobic respiration which causes marked depletion of ATP
¨ Reduced ATP production causes failure of energy dependent pumps which causes cellular swelling, reduction of pH and structural destruction of protein.
¨ Further reduction of oxygen tension causes development of large , amorphous, flocculent densities in mitochondrial matrix
¨ Injury of Lysosomal membrane and leakage of its enzyme
Point of no Return
If hypoxia persists for a certain period different tissues of the body may undergo irreversible damage.
Brain 3-5 min
Heart 30-40min
Kidney 45 min
Liver 1-2 hours
Measurement
- Hb saturation with O2
Oxymetry(SaO2, SpO2)
- O2 Content
Vas Slyke apparatus
- Partial Pressure of Oxygen
Oxygen electrode
- SaO2 and PaO2 are the principal clinical indicators for initiating, monitoring, and adjusting oxygen treatment.
- However SaO2 and PaO2 can be normal in hypoxia caused by low cardiac output, anaemia and Histotoxic hypoxia. In these circumstances PvO2 is better index of tissue oxygenation.
- But PaO2 and PvO2 may be normal in severe hypoxia in single organ. In this case specialized techniques including Tonometry and Oxygen probes are helpful.
Management
Appropriate management of hypoxia depends on treating the underlying cause while providing supplemental oxygen as necessary.
There are some rules of Oxygen therapy:
- Give Oxygen to the patient as much as you can at first and then reduce it, guided by blood gas measurement
- oxygen treatment will work only if the patient have a patent airway
- Definitive treatment of hypoxia depends on the underlying cause; giving oxygen is a holding measure.
Clinical goals of oxygen therapy:
- Treatment of hypoxaemia
- ? work of breathing
- Decrease myocardial work load
When to start?
“American College of Chest Physicians and National Heart Lung and Blood Institute” recommendations for instituting oxygen therapy:
- Cardiac and respiratory arrest
- Hypoxaemia (PaO2<60 mm Hg, SaO2<90%)
- Hypotension (systolic blood pressure <100 mm Hg)
- Low cardiac output and metabolic acidosis (bicarbonate<18 mmol/l)
- Respiratory distress (respiratory rate >24/min)
Oxygen therapy in Anaesthesia
Hypoxia is not uncommon in patient under Anaesthesia and in post operative ward. Oxygen therapy should be given:
Before induction
To enrich FRC
Under anaesthesia
To correct hypoxaemia resulting from:
- Hypoventilation due to Anaesthetic drugs and Opioids
- V/Q mismatch
- ?FRC
- closing volume encroaches VT
During recovery
To prevent
Diffusion Hypoxia
Post Operative
Routine 10 min following GA:
- IHD
- ? CO
- Anaemia
- Obesity
- Hypothermia
- shivering
- Pul Oedema
- Airway obstruction
In post operative ward patient may experience severe hypoxia due Hypoventilation as a result of severe pain. So appropriate management of pain is a part of successful treatment of hypoxia along with oxygen therapy.
Devices
High-Flow OR Fixed-Performance devices: HAFOE, Anaesthetic Breathing System, Ventilator
The delivered FiO2 is not affected by variations in ventilatory level or breathing pattern. These devices are suitable for patients who require:
- A constant FiO2
- Large inspiratory flows of gas (>40L/min)
Variable performance devices: Nasal canula. Face mask
Delivered FiO2 is affected by variations in ventilatory level or breathing pattern.
Low flow systems are adequate for patients with:
- Minute ventilation less than 8-10L/min
- Breathing frequencies less than 20 breaths/min
- Tidal volume less than 0.8 L
- Normal inspiratory flow(10-30 L/min)
Dark sides of Oxygen
- Joseph Priestly
Fire
Oxygen supports combustion of fuels. An increase in the concentration of oxygen from 21% up to 100% causes a progressive increase in the rate of combustion with the production of either conflagrations or explosions with appropriate fuels.
Cardiovascular depression
An increase in PO2 leads to direct vasoconstriction, which occurs in peripheral vasculature and also in the cerebral, coronary, hepatic and renal circulations. This effect is not manifest at PaO2 of less than 30 kPa and assumes clinical importance only at hyperbaric pressures of oxygen. Hyperbaric pressures of oxygen also cause direct myocardial depression. In patients with severe cardiovascular disease, elevation of PaO2 from the normal physiological range to 80 kPa may produce clinically evident cardiovascular depression.
Absorption atelectasis
Because oxygen is highly soluble in blood, the use of 100% oxygen as the inspired gas may lead to absorption atelectasis in lung units distal to the site of airway closure. Absorption collapse may occur in as short a time as 6 min with 100% oxygen, and 60 min with 85% oxygen. Thus, even small concentrations of nitrogen exert an important splinting effect and this accounts for current avoidance of 100% oxygen in estimation of pulmonary shunt ratio (Qs/Q.t) m patients with lung pathology, in whom a greater degree of airway closure would result in greater areas of alveolar atelectasis. Absorption atelectasis has been demonstrated in volunteers breathing 100% oxygen at FRC; atelectasis is evident on chest radiography for a period of at least 24 h after exposure.
Co2 narcosis
In patients with chronic bronchitis and chronic CO2 retention, there may be loss of sensitivity of the central chemoreceptors and some dependence of ventilation on drive from the peripheral chemoreceptors that respond to oxygen. Administration of a high .FiO2 to such a patient may cause loss of peripheral chemoreceptor drive with the subsequent development of ventilatory failure.
Pulmonary oxygen toxicity
Chronic inhalation of a high inspired concentration of oxygen may result in the condition termed pulmonary oxygen toxicity (Lorrain-Smith effect), which is manifest by hyaline membranes, thickening of the interlobular and alveolar septa by oedema and fibroplastic proliferation. The clinical and radiological appearance of these changes is almost identical to that of the acute respiratory distress syndrome. The biochemical mechanisms underlying pulmonary oxygen toxicity probably include:
- Oxidation of SH groups on essential enzymes such as coenzyme A
- Peroxidation of lipids; the resulting lipid peroxides inhibit the function of the cell
- Inhibition of the pathway of reversed electron transport, possibly
by inhibition of iron and SH-containing flavoproteins.
These changes lead to loss of synthesis of pulmonary surfactant, encouraging the development of absorption collapse and alveolar oedema. The onset of oxygen-induced lung pathology occurs after approximately 30 h exposure to a PO2 of 100 kPa.
Central nervous system oxygen toxicity
Convulsions(Paul Bert effect), similar to those of grand mal epilepsy, occur during exposure to hyperbaric pressures of oxygen.
Retrolental fibroplasias
Retrolental fibroplasia (RLF) is the result of oxygen-induced retinal vasoconstriction, with obliteration of the most immature retinal vessels and subsequent new vessel formation at the site of damage in the form of a proliferative retinopathy. Leakage of intravascular fluid leads to vitreoretinal adhesions and even retinal detachment. Retrolental fibroplasia occurs in infants exposed to hyperoxia in the paediatric intensive care unit and is related not to the FiO2 per se, but to an elevated retinal artery PaO2. It is not known what the threshold of PaO2 is for the development of retinal damage, but an umbilical arterial PaO2 8-12 kPa (60-90 mmHg) is associated with a very low incidence of RLF and no signs of systemic hypoxia. It should be stressed, however, that there are many factors involved in the development of RLF in addition to arterialhyperoxia.
Depressed haemopoiesis
Long-term exposure to elevated FiO2 leads to depression of haemopoiesis and anaemia.
Oxygen induced cell injury
The overzealous and unregulated use of supplemental oxygen must be tempered by the potential for oxygen to act as a powerful and even lethal toxin. In fact, contrary to the notion that oxygen protects cells from injury, the accumulated evidence suggests that oxygen (via the production of toxic metabolites) is responsible for much of the cell injury in critically ill patients. The following is a brief description of the dark (toxic) side of oxygen.
The intermediates in oxygen metabolism:
Superoxide radical
Hydrogen peroxide
Hydroxyl Radical.
Overzealous and unregulated use of oxygen must be tempered for the potential of it’s to act as a potential or even lethal toxin.
References:
1. http://www.free-medical-books.webs.com
2. The ICU book
3. clinical Anesthesia morgan
Article By: Dr. Md. Rajib Pervez
History of Telomere and Telomerase
Painless Knee Replacement Surgery! Is It Possible?
Effectiveness of Lauric Acid and Adrographis Extract on Skin Pathogens
ART Laboratory and ART Equipments
Commonly found IBD symptoms
When Eyes Cry: The Cure to Dry Eyes
Lipoprotein lipase for treating Atherosclerosis.
Use of Statistics in Hospital and Healthcare Organizations
Impact of Clinical Pharmacist in an Anticoagulation Management Service in several countries
Abnormal Heart Rate Recovery Immediately After Treadmill Testing : Correlation with Clinical, Exercise Testing, and Myocardial Perfusion Parameters
Application of Statistics in Hospital and Healthcare Organizations
A Polypill Offering Empty Hope
Diabetes Mellitus
LASIK and sports-related eye injuries
anaemic hypoxia
,anaemic hypoxia management
, symptoms and treatment of post op hypoxia, hypoxia during anesthesia, causes of hypoxia during general anaesthesia, what pao2 constitutes hypoxia,signs and symptoms of hypoxia after anesthesia
,post operative hypoxia and bradycardia
, ,oxygen cascade and its importance in anesthesia
,severe hypoxia under anesthesia
, ,hypoxia anaesthesia causes signs management
,symptoms of post operative hypoxia
, , , , ,hypoxia under anaesthetic management
, , , , , ,hypoxia anesthesia induction case study
,causes of inspiratory gas with co2 during general anaesthesia
,hypoxia causes during anesthesia
, , ,hypoxia under anesthesia signs and symptoms
,hypoxia during general anesthesia in children
,causes of hypoxia during anaesthesia
, ,signs of hypoxia with anesthesia
, , , , , ,under anaesthesiacauses of hypoxia in children
, ,hypoxia in postoperative patients
, , , ,hypoxia under anaesthesia and icu
, , , , ,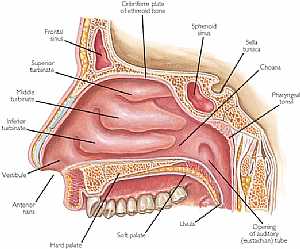 Nose anatomy
Nose anatomy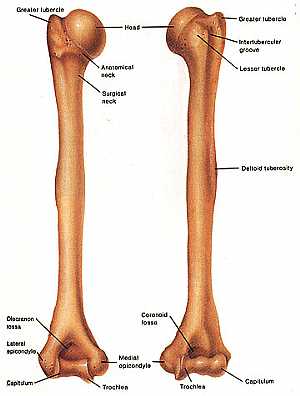 Humerus bone
Humerus bone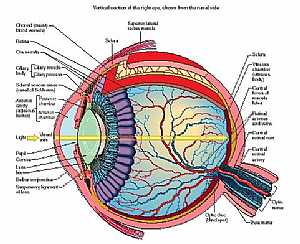 Eye anatomy
Eye anatomy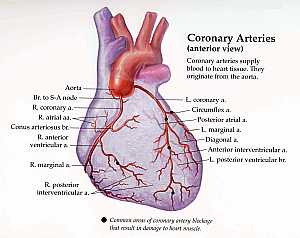 Coronary arteries anatomy
Coronary arteries anatomy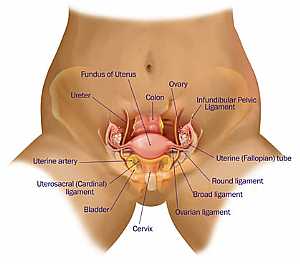 Female pelvic anatomy
Female pelvic anatomy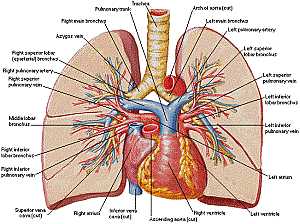 Heart and lung anatomy
Heart and lung anatomy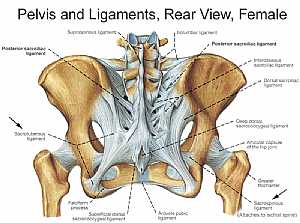 Bones and ligaments of the FEMALE Pelvis
Bones and ligaments of the FEMALE Pelvis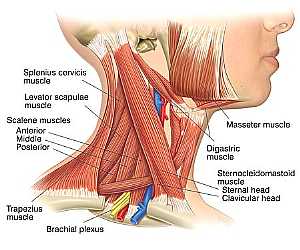 Neck Anatomy
Neck Anatomy MidBrain anatomy
MidBrain anatomy Oral Cavity
Oral Cavity Stomach anatomy
Stomach anatomy Lung anatomy
Lung anatomy Basal Cell Carcinoma ("Rodent Ulcer" Type)
Basal Cell Carcinoma ("Rodent Ulcer" Type)
 Basal Cell Carcinoma ("Rodent Ulcer" Type)
Basal Cell Carcinoma ("Rodent Ulcer" Type) Basal Cell Carcinoma (Histology-Morpheaform Type)
Basal Cell Carcinoma (Histology-Morpheaform Type)
 Basal Cell Carcinoma (Histology-Morpheaform Type)
Basal Cell Carcinoma (Histology-Morpheaform Type) Basal Cell Carcinoma (Histology-Nodular Type - High power)
Basal Cell Carcinoma (Histology-Nodular Type - High power)
 Basal Cell Carcinoma (Histology-Nodular Type - High power)
Basal Cell Carcinoma (Histology-Nodular Type - High power) Basal Cell Carcinoma (Histology-Nodular Type- High power)
Basal Cell Carcinoma (Histology-Nodular Type- High power)
 Basal Cell Carcinoma (Histology-Nodular Type- High power)
Basal Cell Carcinoma (Histology-Nodular Type- High power) Skin
Skin
 Skin
Skin Nervous System -- Basic
Nervous System -- Basic
 Nervous System -- Basic
Nervous System -- Basic Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy Head anatomy
Head anatomy
 Head anatomy
Head anatomy Brain anatomy
Brain anatomy
 Brain anatomy
Brain anatomy© Copyright 2001-2022 eDoctorOnline.com
i think this is a perfect article on hypoxia.